Medical ethics, also known as bioethics, is an amalgam of medicine, law, and religion. It is also influenced by cultural beliefs. In this course, we will define the most common ethical principles and note their relationship to the basic theories of ethics. Some of the prominent court cases that have dictated the basis of physician-patient relationships, especially in end-of-life care, are presented. Also, the Patient Self-Determination Act is outlined with explanations of advance directives—better known as physician directives and durable power of attorney for health care. Finally, a possible method of setting up a workable ethical decision-making framework is presented in some detail. Hopefully this will be unseful in the event of a conflict or when a decision involving ethical issues confronts us or our fellow physicians. This course should allow us to comprehend the basic precepts of medical ethics and afford us the general knowledge of how to apply them in our everyday practice of medicine.
- INTRODUCTION
- BRIEF HISTORY OF BIOETHICS
- LANDMARK COURT CASES
- PATIENT SELF-DETERMINATION ACT (PSDA) OF 1990
- DEFINITIONS OF ETHICAL PRINCIPLES
- ETHICS AND THE DECISION-MAKING PROCESS
- ETHICAL THEORETICAL SYSTEMS
- PRACTICAL APPLICATION OF ETHICAL THEORIES
- SETTING UP A WORKABLE ETHICAL DECISION-MAKING FRAMEWORK
- PHYSICIAN-ASSISTED SUICIDE
- AMA CODE OF ETHICS
- CONCLUSION
- RESOURCES
- Works Cited
This course is designed for physicians and interested healthcare professionals.
The purpose of this course is to briefly review the history, theory, and practical application of ethical principles to issues that arise in clinical practice. The goals of the course are to heighten awareness and promote self-reflection, address knowledge gaps, improve communication and decision-making skills, and promote reasonable, humane care for patients and families.
Upon completion of this course, you should be able to:
- Outline the history of bioethics, including the evolution of the physician-patient relationship.
- Discuss the Karen Ann Quinlan and Nancy Cruzan cases as they influenced national and state healthcare policies.
- State the purpose of the Patient Self-Determination Act (PSDA) of 1990 and the role of healthcare professionals.
- Differentiate between the types of advance directives.
- Discuss the national ethical standards frameworks and their relationship to ethical decision making for patients.
- Define terminology regarding bioethics, including the principles guiding medical ethical decision making.
- Compare and contrast various ethical theories as they relate to health care.
- Describe elements of setting up a workable ethical decision-making framework.
John M. Leonard, MD, Professor of Medicine Emeritus, Vanderbilt University School of Medicine, completed his post-graduate clinical training at the Yale and Vanderbilt University Medical Centers before joining the Vanderbilt faculty in 1974. He is a clinician-educator and for many years served as director of residency training and student educational programs for the Vanderbilt University Department of Medicine. Over a career span of 40 years, Dr. Leonard conducted an active practice of general internal medicine and an inpatient consulting practice of infectious diseases.
Contributing faculty, John M. Leonard, MD, has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
John V. Jurica, MD, MPH
The division planner has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
Sarah Campbell
The Director of Development and Academic Affairs has disclosed no relevant financial relationship with any product manufacturer or service provider mentioned.
The purpose of NetCE is to provide challenging curricula to assist healthcare professionals to raise their levels of expertise while fulfilling their continuing education requirements, thereby improving the quality of healthcare.
Our contributing faculty members have taken care to ensure that the information and recommendations are accurate and compatible with the standards generally accepted at the time of publication. The publisher disclaims any liability, loss or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents. Participants are cautioned about the potential risk of using limited knowledge when integrating new techniques into practice.
It is the policy of NetCE not to accept commercial support. Furthermore, commercial interests are prohibited from distributing or providing access to this activity to learners.
Supported browsers for Windows include Microsoft Internet Explorer 9.0 and up, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Supported browsers for Macintosh include Safari, Mozilla Firefox 3.0 and up, Opera 9.0 and up, and Google Chrome. Other operating systems and browsers that include complete implementations of ECMAScript edition 3 and CSS 2.0 may work, but are not supported. Supported browsers must utilize the TLS encryption protocol v1.1 or v1.2 in order to connect to pages that require a secured HTTPS connection. TLS v1.0 is not supported.
The role of implicit biases on healthcare outcomes has become a concern, as there is some evidence that implicit biases contribute to health disparities, professionals' attitudes toward and interactions with patients, quality of care, diagnoses, and treatment decisions. This may produce differences in help-seeking, diagnoses, and ultimately treatments and interventions. Implicit biases may also unwittingly produce professional behaviors, attitudes, and interactions that reduce patients' trust and comfort with their provider, leading to earlier termination of visits and/or reduced adherence and follow-up. Disadvantaged groups are marginalized in the healthcare system and vulnerable on multiple levels; health professionals' implicit biases can further exacerbate these existing disadvantages.
Interventions or strategies designed to reduce implicit bias may be categorized as change-based or control-based. Change-based interventions focus on reducing or changing cognitive associations underlying implicit biases. These interventions might include challenging stereotypes. Conversely, control-based interventions involve reducing the effects of the implicit bias on the individual's behaviors. These strategies include increasing awareness of biased thoughts and responses. The two types of interventions are not mutually exclusive and may be used synergistically.
#47175: Medical Ethics for Physicians
In today's ever-changing societal and healthcare environments, physicians are confronted with choices concerning what is best for their patients, their practice, their institution, or themselves; such choices often impose ethical considerations that challenge the physician to render a decision in accordance with the principles and values of the profession. These choices can become enmeshed in ethical dilemmas that emerge from conflicting values or administrative rules and legalities. Ethics issues range from the extraordinary, such as end-of-life decisions, to the mundane, such as whether to accept certain gifts from a pharmaceutical company, but all require some understanding of the ethical principles that govern best professional practice and test one's resolve to act in accordance with these values. When ethical dilemmas or conflicts of interest do arise, it is useful to be well informed as to how similar issues have been adjudicated in the past and what tools are at hand to assist in the decision-making process.
The precepts and principles contained within various ethical systems can assist in conceptualizing a problem-solving approach allied in resolving an ethical dilemma. Whether decision-making involves an individual facing end-of-life choices or an institution setting administrative policies, these systems and principles can help the healthcare professional clear the blurred lines that may develop in difficult ethical situations. For example, if a known user of illicit drugs demands opioid pain management, how then should appropriate treatment choices be made by those responsible for care? Other examples of potential management dilemmas might be an individual with alcohol use disorder needing a liver transplant, a patient with diabetes who seemingly refuses to adhere to a diet protocol, a sedentary businessman who resists lifestyle changes necessary for cardiovascular risk reduction, or a physician whose stress level is beyond the coping stage.
Oftentimes, the patient's aspirations or goals may not correspond with what the family or physician believes would be best. Even between seemingly alike individuals, with similar education and background, value systems may prove to be radically different. Consider the patient who refuses life support while the family insists they want every lifesaving measure taken, or conversely, the comatose patient whose family members want life support and other interventions stopped, even as the physician refuses to discontinue therapy.
Until fairly recently, the majority of clinical and ethical decisions in medicine were made by physicians acting in a paternalistic manner toward their patients. Questions regarding many issues, such as organ transplantation, assisted life support, patient self-determination, appropriation of dialysis, in-vitro fertilization, cloning, and even the use of generic drugs, did not arise. The reason is simple: these techniques and procedures were not available.
In order to better understand contemporary medical ethics, it is helpful to look back at how ethical principles, frameworks, and/or codes have evolved over centuries. More specifically, it is important to recall several 20th century events in research and medicine that solidified the need for the study and application of ethics and led to the emergence of the field of bioethics. The following pages present a brief discussion of some of the information regarding ethical issues in medicine as it pertains to the role of physicians in the 21st century.
Bioethics is a relatively new field that emerged in the 1960s, prompted in part by rapid technologic advances in medicine and the subspecialization of clinical care. The advent of antimicrobial and cancer chemotherapy, valve and joint replacement surgeries, and organ transplantation provided the means to greatly improve outcomes and prolong life but added new complexities to the clinical decision-making process. The convergence of modern means and rising healthcare costs created the need to talk about how medical and healthcare regulations should be made, who should make them, and what their implications might be for the long term. In the late 1960s, philosophers, theologians, physicians, lawyers, policy makers, and legislators began to write about these questions, hold conferences, establish institutes, and publish journals for the study of bioethics. In 1969, the Institute of Society, Ethics, and the Life Sciences was established at Hastings-on-the-Hudson, New York. Two years later, the Kennedy Institute of Ethics was established at Georgetown University, in Washington, DC.
Prior to the 1960s, medical care decisions were part of the paternalistic role of physicians in our society. Patients readily acquiesced care decisions to their physicians because they were regarded almost as family. What drove this resolve of patients to acquiesce their medical care and treatment decisions to their physicians? David Rothman, as discussed in his book, Strangers at the Bedside: A History of How Law and Bioethics Transformed Medical Decision Making, believes physicians were given such latitude by their patients because they were well-known and trusted by their patients and the community in which they practiced [1]. There were essentially no specialists. One physician took care of a patient and family for a lifetime. The frontier physician often knew the patient from birth to adulthood, made house calls, and was a family friend who knew best what the patient should do with a healthcare concern. Since the 1960s, physicians have generally become strangers to their patients.
The trend away from the family doctor making all the healthcare decisions toward a healthcare system replete with specialists, policy makers, ethical codes, administrative codes, and informed consent was brought about largely by three events in U.S. History. First, World War II research and experimentation (e.g., experimentation on concentration camp prisoners by the Nazis, research on atomic bomb survivors) brought attention to people as test subjects and what rights should be recognized on their behalf. Second, the modern structuring and organization in healthcare delivery moved patients from their familiar surroundings of home and neighborhood clinics to the often intimidating, large hospital. Third, the medical technologic boom brought life-saving interventions; people now live longer due to major advances, such as improved diagnostic procedures, antibiotics, new surgical techniques, and vaccines.
Extensive publicity about three research projects resulted in the establishment of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. The first project involved elderly patients with chronic illness who were injected with live cancer cells in an effort to discover whether the cells would survive in a person who was ill but did not previously have cancer. No consent was obtained from patients or family members before proceeding.
The second project began in 1932, when the Public Health Service initiated a syphilis study on 399 black men from Tuskegee, Alabama. The goal of the study was to observe the men over a period of time to examine how the disease progressed in individuals of African descent. When the study began, there was no cure for the disease; however, fifteen years into the study, penicillin was discovered to be a cure for syphilis. The research participants were never informed, and treatment was withheld in spite of the fact that by the end of the experiment in 1972, 128 men had died either from the disease or related complications [2].
Finally, in 1967, children with mental retardation at the Willowbrook State School, New York, were given hepatitis by injection in a study that hoped to find a way to reduce the damage done by this disease. Although consent was obtained in this study, the consent sometimes had an element of coercion. Gaining admission to the school was difficult and parents were given a guarantee their child would be admitted if they consented to the participation of their child in the study.
In response to these events, the National Commission for the Protection of Human Subjects was created in 1974 by public law. Finally, in 1979, the commission published The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research [3]. This commission recommended that all institutions receiving federal research funding should establish institutional review boards (IRBs). These boards, made up of researchers and lay people, were to review biomedical and behavioral research proposals to ensure that they met ethical standards for protecting the rights of the potential subjects. For many, this was an initial entry into what would later be called bioethics.
In 1973, the first edition of the Hastings Center Studies pointed out the problems they felt were most important to consider when developing healthcare research projects [4]. Remarkable advances were projected in the areas of organ transplantation, human experimentation, prenatal diagnosis of genetic disease, the prolongation of life, and control of human behavior. All of these had the potential to produce difficult problems, thus requiring that scientific knowledge be matched by ethical insight.
Soon, the federal government, private philanthropists and foundations, universities, medical schools, and committed professionals moved quickly to address these questions. The federal government supported programs through the National Science Foundation's Ethics and Values in Science and Technology (EVIST) and the National Endowment for the Humanities, which developed applied medical ethics courses for medical students and college undergraduates. Universities established departments, institutes, and programs in bioethics, including some in which graduate studies could be pursued. Professional organizations (including local bar and medical associations) began to establish committees to look at ethical issues in healthcare. In addition, such interdisciplinary organizations as the Society for Health and Human Values came into existence, including among their members physicians, nurses, social workers, attorneys, theologians, and philosophers.
Hospitals also began to consider how bioethical concerns affected the care they provided patients. In 1976, the Massachusetts General Hospital Critical Care Committee published its recommendations for treating hopelessly ill patients and for using critical care facilities. In Catholic hospitals, committees were formed not only to discuss such specific care issues as sterilization, but also to consider the more general question of how Catholic values should be implemented in their hospitals.
In November 1978, The President's Commission for the Study of Ethical Problems in Medicine and Medical and Biobehavioral Research was created [5]. Its members began work in January 1980. The United States Congress charged them with conducting studies and reporting on a number of topics, including the definition of death, informed consent, and access to healthcare. By spring 1984, the commission had published nine reports addressing many of the problems facing the healthcare system.
These reports stand as a foundation for the organized and socially sanctioned study of the ethical implications of high-technology medical care and ethical regulation of the healthcare industry. The remainder of the 1980s and early 1990s saw continued emphasis on the protection of individual rights. However, more attention began to be paid to the allocation of resources and the effectiveness of complex treatments, especially in terms of the quality of life associated with the prolonging of lives.
The President's Commission, like the National Commission for the Protection of Human Subjects before it, established a model for finding consensus and for articulating ethical conflicts when consensus could not be found. They did for the nation what each ethics committee does for its own hospital or individual health agency.
It was during these transitional years that ethics, law, and medicine began to form an alliance. The legal and medical professions were often on opposite sides of an issue. However, they found themselves increasingly working toward the same goals.
It was the New Jersey Supreme Court Decision in the Karen Ann Quinlan case that brought bioethics to the level of the individual through the media and transformed physician paternalistic authority into patient-physician shared decision making [6]. Patient autonomy issues came into public focus in the 1970s when the legal community set a precedent for deciding withdrawal/withholding of life-sustaining treatment. Although there were many related cases with decisions on medical treatment and decision making for competent and incompetent patients, two cases are recognized as landmark cases and were the most important in influencing the medical and legal community. These two cases were most responsible for moving the primary healthcare decision making into the hands of the individual. These court cases are the previously mentioned New Jersey Supreme Court Decision in the Matter of Karen Ann Quinlan (1976) and the U.S. Supreme Court Decision in the Matter of Nancy Cruzan (1990) [7]. From these two cases, and more specifically from the Nancy Cruzan case, the Patient Self-Determination Act (PSDA) of 1990 was enacted [8].
In the case of Karen Ann Quinlan, the concept of acknowledging a patient's right and the family's right to speak for an individual came to the public via the televised and printed news media. The plight of Karen and her parents began in 1975 when she presented at the local hospital, unconscious, possibly from ingestion of a mixture of alcohol and barbiturates. Placed on a ventilator and with little hope of regaining consciousness, her physicians related this grim prognosis to Karen's parents. Karen's father went to the New Jersey court requesting he be made his daughter's guardian and in so doing would be permitted to consent (for her) to discontinue ventilator support. The New Jersey Attorney General and the County Prosecutor stood firmly embedded in their advisement that to remove the ventilator from Ms. Quinlan constituted criminal homicide. Medical experts testified that under the current "medical standards, practice, and ethics," the ventilator must be continued [6].
Mr. Quinlan asserted that his daughter's right of privacy was justification for the request to terminate life support, and the court accepted the relevance of this right both to the treatment termination decision and to Mr. Quinlan's right to assert his daughter's right to privacy. In this way the court eliminated the issue of criminal homicide.
Despite the court's acknowledgment of autonomy, it did not permit that right as the basis for a decision to terminate the treatment. However, the court did decree that if an ethics committee agreed with Quinlan's physicians that there was "no reasonable possibility of Karen's ever emerging from her present comatose condition," and if the family and Ms. Quinlan's guardian agreed, the ventilator could be withdrawn [6]. The expectation was that Karen would die following the weaning off the ventilator. In fact, Ms. Quinlan was successfully weaned off the ventilator and lived until June 1985. However, she never regained consciousness in that time.
The Karen Ann Quinlan case is significant because it was the first case to deal specifically with the question of withdrawing ventilator support from a permanently unconscious patient. It is often cited as a source for the importance of the "privacy right" in life and death decisions.
In 1983, Nancy Cruzan presented to the local hospital in a comatose state, a result of an automobile accident that left her in a persistent vegetative state (PVS). What links Ms. Cruzan's case to the principle of the patient's autonomy (and subsequently to issues of right to die) and to the Karen Ann Quinlan case is the fact that neither individual could speak for herself once the actual situation requiring a decision presented itself. Therefore, the two cases are linked by the fact that family members went forward to speak for the individuals.
The difference between this and the Quinlan case is that a feeding tube, and therefore continuation of artificial feeding and hydration, was the central focus and seemed to be viewed differently than other life-sustaining treatment measures. The Cruzan parents fought to have the artificial feeding tube removed from their daughter. Nancy was not comatose in the common sense, yet not able to function on her own. To many, PVS was not seen as synchronous with terminal illness. As a result, the court determined that only if there was proof by clear and convincing evidence that she (Nancy Cruzan) authorized such treatment (or rejection of it) prior to losing her decision-making capacity would they rule to discontinue the tube feeding.
Through other case decisions, it had been determined that competent and incompetent patients alike had the same rights of decision making under specific circumstances. As long as the now incompetent individual had provided evidence at an earlier time of her life, while competent, of what healthcare decisions she would make under specific conditions, her voice could be heard as if she was competent and making the decision during the present time.
The first ruling came on July 27, 1988 from Judge Charles Teel of the Missouri court who agreed with the parents and, acting for Nancy Cruzan, now a ward of the court, gave permission to have the feeding tube removed. However, in a 4-3 decision by the Missouri Supreme Court on November 16, 1988, that ruling was overturned and upheld in the U.S. Supreme Court on June 25, 1990. Their reason for overturning Judge Teel's decision was there had been no clear, convincing evidence that Nancy Cruzan had indicated verbally or in writing what her prior wishes would have been in the situation she now experienced.
On December 14, Judge Teel once again sustained his decision to allow the discontinuance of the artificial feeding and hydration tube. The difference between his first and final judgments was the new "clear and convincing evidence," required by the State, which was brought forward on November 1 by three new witnesses. These witnesses were friends of Nancy Cruzan who testified for the first time that she had told them many years before that she would have wanted to terminate the tube feeding if she was in a situation like the present one. The "clear evidence" was presented in three points made by Judge Teel [7]:
"That the intent of our ward, if mentally able, would be to terminate her nutrition and hydration."
"That there was no evidence of substance to cause belief that our ward would continue her present existence, hopeless as it is, and slowly progressively worsening."
"That the co-guardians, Lester L. and Joyce Cruzan, are authorized to cause the removal of nutrition and hydration from our ward, Nancy Beth Cruzan."
It is important to emphasize that the U.S. Supreme Court's ruling does not require all states to mandate clear and convincing evidence of anything before life support may be terminated. Each state remains free to set its own standard of proof. Each state may decide to require or not to require clear and convincing evidence of the incompetent individual's previously determined wishes.
Over the years, from the Quinlan and Cruzan cases to the many others (including the more recent Schiavo case) that address patients' rights to refuse treatment and the idea of who can speak for incompetent patients, state courts began to address the issues explicitly. Multiple states reached substantial agreement that:
Competent patients have a constitutional and common-law right to refuse treatment.
Incompetent patients have the same rights as competent patients.
The interests of the state opposing this right are virtually nonexistent in the case of competent patients and very weak in the case of incompetent patients whose prognosis for recovery is dim.
The decision-making process should generally occur in the clinical setting without resort to the courts, which are available to assist in decision making when an impasse is reached.
In making decisions for incompetent patients, surrogate decision makers should effectuate the patient's own preferences expressed before the patient lost decision-making capacity (the subjective standard); however, if these references are not known, the surrogate, based on whatever evidence is available, should approximate what the patient would have wanted (the substituted judgment standard). If there is no information about the patient's preferences, the surrogate should make a decision that is in the patient's best interests (the best interests standard).
In ascertaining an incompetent patient's preferences, the attending physician and surrogate may rely on the patient's "advance directive," which may be written or oral.
Artificial nutrition and hydration are medical treatments and may be withheld or withdrawn under the same conditions as any form of medical treatment.
The Nancy Cruzan case was the ultimate landmark decision that led to legislation that would give legal rights to individuals to make healthcare decisions for themselves. Those decisions could then be written down as directives for use in the future should the individual not be able to speak for him or herself and found to be in a healthcare situation requiring decisions regarding further treatment choices (or refusal of such) in the life of that individual. This legislative act became known as the Patient Self-Determination Act of 1990.
Although this multi-state consensus was not without exception, these were the precursor principles to the PSDA of 1990, a federal law given over to the states to implement as of December 1, 1991 [8]. This new legislation applied to hospitals, nursing homes, hospice, HMOs/PPOs, and any other facilities that received funds from Medicare or Medicaid programs. It mandated that each of the affected facilities must advise their patients of their legal rights and options for accepting or refusing treatment if they (the patients) should become unable to speak for themselves. The primary provisions of the PSDA are:
Providers must offer written information and summaries of pertinent institutional policies to all adult patients regarding their rights under state laws to accept or refuse treatment and to make advance directives.
The patient's record must be documented to indicate whether the patient has an advance directive.
Institutions may not discriminate against or refuse care to a patient based upon whether the patient has executed an advance directive.
Institutions have an affirmative obligation to comply with requirements of state law regarding advance directives.
Institutions must provide (individually or with others) education to staff and community regarding issues associated with advance directives.
State Medicaid laws must be amended to require participating healthcare institutions to furnish the written information mentioned above.
With the Department of Health and Human Services' assistance, state Medicaid agencies must develop written descriptions of state laws on advance directives, and these materials are to be distributed by participating healthcare institutions.
Finally, legislation was created to keep end-of-life medical decision-making issues out of the courts and in the appropriate arena, with the appropriate players: the patient/family and the healthcare professionals. The central focus of the law is the provision of patient education. The means or the tool for the individual to document his or her wishes for future healthcare decisions is called an advance directive. There are two types of advance directives available. Although both are not required to be completed together, most people are encouraged to do so.
The first type of advance directive is called a physician directive, sometimes called directive to physician. The precedent form is the living will, an earlier, legally non-binding form. The living will allowed an individual to state his/her treatment choices should he or she be found in a terminal state, comatose, and/or in another condition leading to imminent death for which the physician saw no cure. The patient stated that he/she be allowed to die naturally without medical intervention, with only comfort measures employed.
To this statement or its facsimile, this form does have a clause exempting any pregnant mother from having this advance directive honored while she remains in a pregnant state. Another clause may be added regarding the individual's agreement or non-agreement to the discontinuance of artificial feeding and hydration through a feeding tube (adopted from the Nancy Cruzan case decision).
The directive is signed by the individual and is honored only if the patient meets the criteria set forth in the advance directive. It is the clear and convincing evidence required by some states that the individual initiates and signs this form while competent, and his or her signature (usually required to be notarized or witnessed by two witnesses) affirms this.
The second type of advance directive is known as a durable power of attorney for health care (DPAHC) and allows the individual to choose another person to act on his or her behalf should the individual become incapacitated and unable to do so, at any future time. This document offers more comprehensive choices for the individual by giving more scenarios and noting the patient's wishes in those situations in the future. The DPAHC states the individual's wishes in writing, as does the physician directive, but goes further into the circumstances under which future healthcare decisions may need to be made. It also allows another (a surrogate, also called an attorney-in-fact) to act on the patient's behalf. The named person becomes equal to the patient in terms of his or her right to receive the same information required for decision making. This form also must be signed by the individual and notarized or witnessed.
In both cases, the physician directive and the DPAHC are legal documents in all states and require all healthcare institutions to honor them if the patient meets the criteria. Healthcare agencies must have policies and procedures that allow the process for patient self-determination rights to be honored.
The purpose of the PSDA is to communicate and protect patients' rights to self-determination in health care. The underlying assumptions of the PSDA are that [8]:
Patients who are informed of their rights are more likely to take advantage of them.
If patients are more actively involved in decisions about their medical care, then that care will be more responsive to their needs.
Patients may choose care that is less costly.
From 1991, when the PSDA was first implemented, to today, most individuals have not completed advance directives and/or do not have them when they enter healthcare agencies that fall under the umbrella of the PSDA. What does this mean for those working in the healthcare field? A method of making an easier end-of-life decision is available, but not often used by the patient. Conflict between patient autonomy and physician paternalism, poor communication, institution or physician fear of litigation, and/or family disagreement with the patient or healthcare professionals continues to be an issue. More policies or guidelines are being adopted to assist the process so that, even when advance directives are unavailable, dialogue can be initiated with family members who can legally act for their loved ones. It does not address the cases where the DPAHC surrogate is a non-relative and relatives disagree with the surrogate, and therefore, the patient's wishes. It does not settle satisfactorily the right of the significant other, the named surrogate vs. his sibling, or the present wife vs. the ex-wife, who wishes to make decisions for the patient without an advance directive. Those cases make for interesting studies but hopefully can be decided by directives from hospital policy regarding who can speak for the individual without an advance directive.
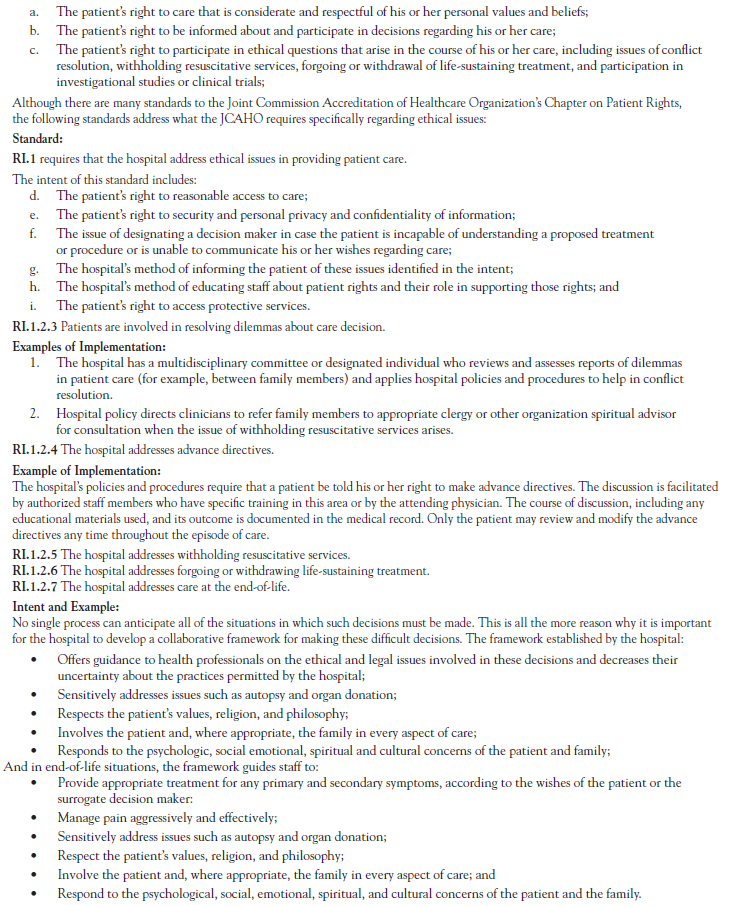
Many situations require only listening and someone to support the patient and family through the process of decision making. The Joint Commission has established standards on patient rights, including ethical decision making. Very clearly, the Joint Commission has outlined that hospitals should have defined policies and procedures allowing patients to create and modify advance directives. The 2000 Joint Commission Standards regarding patients' rights to formulate an advance directive, to have a mechanism in place to deal with ethical issues, and for their rights to accept or refuse care, is found in Figure 1. Because the information in Figure 1 presents so many useful concepts in a single page, it remains a part of this course although it is no longer contained in the current Joint Commission manual [9].
This form has since been replaced with an entire section titled "Rights and Responsibilities of the Individual," which appears in the 2025 revision of the Comprehensive Accreditation Manual for Hospitals published by the Joint Commission [9]. This section outlines the standards that healthcare organizations must follow in order to obtain or maintain accreditation. The expanded standards section makes it easier for healthcare organizations to test their compliance and for reviewers to rate them.
The Joint Commission requires healthcare organizations to follow their state laws. If a person is from out of state, they may have an advance directive that does not comply with the state laws where the patient is hospitalized. Some attorneys advise hospitals treating patients who bring advance directives from out-of-state to ask them to complete an advance directive for the state in which they are being treated. What if the patient presents to a hospital in a coma? The hospital must work with the advance directive provided. Some states allow surrogate decision makers for patients under certain conditions, such as terminal illness or vegetative state. Those laws usually require the physician to certify that the patient meets the medical conditions before allowing a surrogate decision maker to step in. When there is no advance directive, some states allow the patient's spouse or adult children (or other direct relatives listed in a specified order of preference) to decide for the patient.
The major ethical principles of significance to physicians and other healthcare personnel are respect for persons, autonomy, veracity, beneficence, non-maleficence, justice, fidelity, and right-to-know [10]. These terms are used widely in bioethics and should be briefly defined:
Respect for persons requires that each individual be treated as unique and be entitled to treatment that is respectful of their human dignity.
Autonomy refers to the right of the patient to determine what will be done with his or her own person. It also involves the patient's right to have confidentiality of their own medical history and records, and for the medical personnel to safeguard that right.
Veracity involves truthfulness. Physicians are obligated to be truthful with patients and/or their families and should avoid withholding information. This allows them to make informed choices.
Beneficence refers to the ethical principle of doing or promoting good.
Non-maleficence correlates to Hippocrates' principle of doing no harm.
Justice is broadly understood as fairness; however, it pertains to what someone or a group is owed. It also relates to the distribution or allocation of a scarce resource or treatment. The principle of justice can also be applied in decisions about end-of-life care, such as the right of the patient to receive adequate palliative treatment.
Fidelity means remaining faithful to promises made.
Right-to-know is the principle of informed consent.
Ethical decision making is the generic term for the process of making a decision within an ethical context in a specific setting (e.g., business, education, or medicine). Ethics are the beliefs an individual or group maintains about what constitutes correct or proper behavior [11]. To put it simply, ethics are the standards of conduct an individual uses to make decisions. The term morality is often confused with ethics; however, morality involves the judgment or evaluation of an ethical system, decision, or action based on social, cultural, or religious norms [11,12]. The word "morals" is derived from the Latin word mores, which translates into customs or values.
The foundation from which ethical principles originated began from debates and discussions in ancient times. These ethical principles then became the theoretical framework upon which actions as individuals and societies are based. Most prominently, the Hebrew biblical covenants and the teachings of Greek philosophers, such as Plato and Aristotle, form the basis for most of the familiar ethics and morals prevalent in Western society today.
How then are theoretical ethics translated into the day-to-day practical application of those principles in today's rapidly changing, technology-driven world? It really boils down to a deductive reasoning process that starts with the broad and generally accepted ideas of what constitutes proper respect for the individual and how people should act within society. Then, the process narrows in focus to a smaller group or individual situation in which the ethical principles serve as a guide for daily living. When a situation presents itself that contradicts the established "norm," it may cause a dilemma. When these dilemmas are of an ethical nature, we often say the situations are controversial or have called into question or infringed upon a group or individual's rights based upon accepted ethical theories and moral practices.
How does one move from general ethical concepts, based on religious or philosophical theoretical frameworks (discussed later in this course), to practical application for patient/society healthcare decision making? Ordinarily, an ethical conflict presents itself when a person's or group's ethical values or principles are challenged or conflict with one another over some decision related to clinical care. It is imperative to identify what principles or values are in conflict so that an appropriate resolution can be made.
A dilemma occurs when one is faced with what is perceived (or is in reality) to be no alternative, only one alternative, or an either/or choice situation. This dilemma scenario leaves the individual with limited, often painful choices. "Have the surgery or die," may be the only two alternatives given to a patient. This can leave the patient immobilized, powerless, feeling subservient and victimized, and with no sense of control. Providing options accompanied by explanation, context, probabilities, and one's professional judgment, while no less dire, may assist the individual by giving him or her a sense of freedom and participation in the decision-making process. Whether an ethical dilemma exists or not should be the first question. It may simply be conflict arising out of poor communication, which is usually resolved when clarification occurs. Once an ethical dilemma or conflict is determined to exist, one can begin a step-by-step process to open the discourse and begin the decision-making process.
There are a myriad of ethical issues facing patients, families of patients, and physicians today. Examples of these issues include organ transplantation, fetal surgeries, infants with severe anomalies, lifesaving surgery, stem cell research, inability to reach health services, and the rationing of healthcare. Still other issues involve competency of healthcare workers, nurse-physician relationships, treating non-compliant patients, and many more situations that apply to individuals or to the nation on a societal level.
One of the most common ethical issues facing healthcare professionals in patient care settings is the withholding or withdrawing of treatment. Most healthcare institutions are required to have policies and procedures in which the rights of the patient/family and the duties of the healthcare professionals are outlined. It is only when there is a conflict between the parties involving value or moral principles that a dilemma may arise. Often, the real problem may be one of three non-ethical related issues: poor communication between the involved parties, an administrative misunderstanding, or a legal ambiguity.
The first step that should be taken is to gather information about the patient's diagnosis, prognosis, and treatment options, followed by the best medical judgments regarding life expectancy and quality of life with or without treatment. This must include a discussion of the risks and side effects of such treatment. Of equal importance, the patient (if legally competent) must be fully informed and have his or her statement of wishes honored.
Should the patient be temporarily or permanently unable to speak for him or herself, the immediate family, if available, should be consulted. As discussed, most statutes on the right to die, withholding and withdrawing life sustaining treatment, and organ donation identify an individual's immediate family member (usually in a specific order of priority) who can speak for the individual. One question to ask the patient, if competent, is whether or not he or she has an advance directive. This is usually accomplished by the nursing staff, but all healthcare professionals should be certain that it has been done. Administrative factors, such as the risk of liability, current institutional policies, and economic factors that affect the individual family, must also be evaluated.
With this information gathered, it should be apparent whether or not a value conflict exists. Many times, just the process of gathering information allows for clarification and for differences to be resolved. If an ethical dilemma ensues, the next step is to articulate the ethical principles that are opposing one another.
There are numerous ethical theories. Six fundamental theories that directly concern healthcare professionals are deontologic, teleologic, motivist, natural law, transcultural, and relative/multicultural ethical theoretical systems. These systems are each made up of principles, precepts, and rules that form a specific theoretical framework to provide the follower with general strategies for defining the ethical actions to be taken in any given situation.
Under the deontologic umbrella, an action is deemed right or wrong according to whether it follows pre-established criteria known as imperatives. An imperative in our language is viewed as a "must do," a rule, an absolute, a black-and-white issue. This is an ethic based upon duty linked to absolute truths set down by specific philosophical schools of thought. As long as the principles dictated by these imperatives are met with dutiful compliance, one is said to be acting ethically.
One of the most significant features of deontologic ethics is found in John Rawls' Theory of Justice, which states that every person of equal ability has a right to equal use and application of liberty. However, certain liberties may be at competition with one another. There are also some principles within the same ethical theoretical system that can conflict with one another. An example of this conflict might involve a decision over allocation of scarce resources. Under the principle of justice, all people should receive equal resources (benefits), but allocation can easily become an ethical dilemma when those resources are scarce.
The precepts in this system of ethical decision making stand on moral rules and unwavering principles. Regardless of the situation at hand, the purest deontologic decision maker would stand fast by a hierarchy of maxims. They are as follows [13]:
People should always be treated as ends and never as means.
Human life has value.
One is always to tell the truth.
Above all in health care, do no harm.
All people are of equal value.
Health professionals making ethical decisions under the deontologic ethical system see all situations within a similar context regardless of time, location, or people. It does not take into account the context of specific cultures and societies [14]. The terminology used in this system of beliefs is similar to that found in the legal justice system. One differentiation is the enforcement of the rights and duties in the legal system that do not exist in the ethical system.
A framework of legislated supportive precepts (i.e., codes of ethics) serves health professionals by protecting them in their ethical practice. However, even these systems of thought will not clearly define the right answer in every situation. Most healthcare professionals do not practice the concept of the means justifies the end if the end outcome is harmful to the patient. When duties and obligations conflict, few will follow a purist deontologic pathway because most people do consider the consequences of their actions in the decision-making process.
An example of this conflict might involve a decision over allocation of scarce resources. Under the principle of justice, all people should receive equal resources (benefits), but is that possible when those resources are scarce? Who then decides which patient does or does not receive those resources?
A well-known deontologic ethical theory is based upon religious beliefs and is known as the theologic ethical theory. The principles of this theory promote a summum bonum, or highest good, derived from divine inspiration. A very familiar principle is to do unto others as you would have them do unto you. One would be viewed as ethically sound to follow this principle within this system of beliefs.
Another deontologic ethical principle is Immanuel Kant's "Categorical Imperative." Kant believed that rather than divine inspiration, individuals possessed a special sense that would reveal ethical truth to them. That ethical truth is thought to be inborn and causes humans to act in the proper manner. Some of the ethical principles to come from Kant will become more familiar as the principles associated with bioethics are discussed. These include individual rights, self-determination, keeping promises, privacy, personal responsibility, dignity, and sanctity of life.
The teleologic ethical theories or "consequential ethics" are outcome-based theories. It is not the motive or intention that causes one to act ethically, but the consequences of the act [15]. If the action causes a good effect, it is said to be ethical. So here, the end justifies the means.
Utilitarianism is the most well-known teleologic ethical theory. This is the principle that follows the outcome-based belief of actions that provide the greatest good for the greatest number of people. So, rather than individual goodness or rightness, this principle speaks for the group or society as a whole. Social laws in the United States are based upon this principle. The individual interests are secondary to the interest of the group at large. There are two types of utilitarianism: act utilitarianism and rule utilitarianism. In act utilitarianism, the person's situation determines whether an act is right or wrong. In rule utilitarianism, the person's past experiences influence one to greatest good. There are no rules to the game; each situation presents a different set of circumstances. This is also referred to as situational ethics. Situational ethics would say that if the act or decision results in happiness or goodness for the person or persons affected, it would be ethically right.
Individuals may choose the utilitarian system of ethics over another because they find it fulfills their own need for happiness, in which they have a personal interest. It avoids the wall of rules and regulations that may cause a person to feel a lack of control. In Western society, the rule of utility is defined by whatever fits the situation and ultimately leads to happiness.
The application of utilitarianism to healthcare decision making has a downside. In making healthcare policy for a nation of people based upon the principle of doing the greatest good for the greatest number, several questions arise. Who decides what is good or best for the greatest number? Is it society, the government, or the individual? For the rest of the people, are they to receive some of the benefits, or is it an all or nothing concept? How does "good" become quantified in healthcare in such concepts as good, harm, benefits, and greatest? Where does this leave the individual trying to make healthcare decisions?
One modern teleologic ethical theory is existentialism. In its pure form, no one is bound by external standards, codes of ethics, laws, or traditions. Individual free will, personal responsibility, and human experience are paramount. Existentialism lends itself to social work because one of the tenets is that every person should be allowed to experience all the world has to offer. A critique of the existential ethical theory is that because it is so intensely personal, it can be difficult for others to follow the reasoning of a healthcare worker, making proof of the ethical decision-making process a concern.
Another modern teleologic ethical theory is pragmatism. To the pragmatist, whatever is practical and useful is considered best for both the people who are problem solving and those who are being assisted. This ethical model is mainly concerned with outcomes, and what is considered practical for one situation may not be for another. Pragmatists reject the idea that there can be a universal ethical theory; therefore, their decision-making process may seem inconsistent to those who follow traditional ethical models.
The motivist would say that there are no theoretical principles that can stand alone as a basis for ethical living. Motivist belief systems are not driven by absolute values, but instead by intentions or motives. It is not the action, but the intent or motive of the individual that is of importance. An example of a motivist ethical theory is rationalism. Rationalism promotes reason or logic for ethical decision making. Outside directives or imperatives are not needed as each situation presents the logic within it that allows us to act ethically.
Natural law ethics, also known as the virtue system of ethics, is a system in which actions are seen as morally or ethically correct if in accord with the end purpose of human nature and human goals. The fundamental maxim of natural law ethics is to do good and avoid evil. Although similar to the deontological theoretical thought process, it differs in that natural law focuses on the end purpose concept. Further, natural law is an element in many religions while at its core it can be either theistic or non-theistic.
In theistic natural law, one believes God is the Creator, and the follower of this belief sees God as reflected in nature and creation. The nontheistic believer, on the other hand, develops understanding from within, through intuition and reason with no belief rooted in God. In either case natural law is said to hold precedence over man-made law.
The total development of the person, physically, intellectually, morally, and spiritually, is the natural law approach. Therefore, ethical decision making should not be problematic, as judgment and action should come naturally and habitually to the individual follower of natural law.
Although appearing to be the perfect approach to all ethical situations requiring decision making, there are some significant drawbacks; for example, a person's maximum potential is relative or subjective. Additionally, what constitutes natural law? The precept to do good and avoid evil leaves a very large space for interpretation. Because it acts largely outside of individual wishes, often separating human life into a set of separate events, it is an impersonal approach, devaluing the focus upon dignity. To some, it is also a rather cold-hearted approach-not making decisions with the individual, but for the individual based upon what others believe to be good for that person. The principle of paternalism would fit within this context.
Another ethical theory is the modern ethical system of thought that centers on the diversity of cultures and beliefs. Therefore, at its core, this ethic assumes that all discourse and interaction is transcultural because of the strengths and differences in values and beliefs of groups within society. This concept has been developed into what has become known as the transcultural ethical theory.
In the last decade, the ethics of caring has become a specific moral focus of nursing. Attention is being paid to the need for cross-cultural ethical issues in both medicine and nursing. The concept of transcultural nursing was penned by M. Leininger and focuses on a comparative analysis of differing cultures, health-illness values, patterns, caring behavior, and nursing care. Decisions are made on the basis of the value or worth of someone by the quality of interrelationships.
These differences of values, beliefs, or ethical principles are present in healthcare environments. They are much more pronounced when the individuals' values differ greatly from those of the healthcare professionals who care for them. This system of ethics is a holistic framework, built around a model of interrelated precepts: transcultural caring dynamics, principles, transcultural context, and universal source.
This transcultural context encourages individuals and global communities to question and to understand beliefs and values. It is only within this context of caring and life experiences that we can understand ethical issues in a culturally diverse society. The outcome for nursing practice is practical reason. In one author's words, "practical reason focuses on interpretation and prudence and centers on the client professional relationship. Technical or practical reasoning focuses on moral judgments reasoned from a professional/controlling perspective and from a traditional principle-based application of principles perspective" [16].
The advantage to the transcultural ethical system is that it folds some of the other ethical systems together while recognizing the differences between people. A disadvantage might be that Western society largely follows the deontologic and teleologic principles that also make up our legal system. Therefore, there may be some difficulty in making decisions based upon other cultural beliefs and values. Our society largely operates on a basis of facts, conclusions, and predetermined, agreed-upon solutions based historically upon Anglo-European ideals. Many healthcare professionals may find difficulty with the transcultural ethics reliance on close inter-relationships and mutual sharing of differences required in this framework of ethical decision making.
The ethical theory of relativism/multiculturalism falls under the postmodernist philosophical perspective and may be referred to as moral relativism [14]. Multiculturalism promotes the idea that all cultural groups be treated with respect and equality [17]. According to ethical relativists, ethical principles are culturally bound, and one must examine ethical principles within each culture or society [14]. The question then becomes how ethical principles that are primarily deontologic and rooted in Western values are applicable in other societies. The challenge of ethical relativism is how to determine which values take precedent [14].
It is important to remember that ethical theories are just that, theories. They do not provide absolute solutions for every ethical dilemma. They do provide a framework for ethical decision making when adjoined to the critical information gathered from patients and families.
In reality, most healthcare professionals combine the theoretical principles that fit best for the particular patient situation. Whenever the physician-patient relationship is established, a moral relationship exists. Though not an inherent gift, moral courage combined with moral reasoning is required in order to reach ethically sound decisions. This is a skill, and moral reasoning must be practiced so it becomes a part of any healthcare professional's life.
Although all ethical systems concern decisions about ethical problems and ethical dilemmas, the decision reached in regard to a specific conflict will vary depending on the system used. For example, a healthcare professional assigned to care for a patient in the terminal stages of acquired immune deficiency syndrome (AIDS) might have strong fears about contracting the disease and transmitting it to his or her family. Is it ethical for him or her to refuse this assignment?
In answering this question on the basis of utilitarianism, one might weigh the good of personal family members against the good of the patient. Based on the greatest good principle, it would be ethical for the healthcare provider to refuse to care for the patient. In addition, because utilitarianism holds that the ends justify the means, preventing the spread of human immunodeficiency virus (HIV) to the worker's family would justify refusal of the assignment.
Applying deontology to the question, duty and justice are the underlying and unchanging moral principles to follow in making the decision. A person who becomes a healthcare worker accepts the obligations and duties of the role. Caring for patients with infectious diseases is one of those obligations; therefore, refusal would be a violation of this duty. In this system, another unchanging moral principle, justice, would require healthcare professionals to provide adequate care for all patients. Refusing to care for a patient with AIDS would violate this principle.
According to the natural law system, refusing to care for a patient with AIDS would be unethical. One of the primary goals of the natural law system is to help the person develop to maximum potential. Refusing to have contact with the patient with AIDS would diminish the patient's ability to develop fully. A good person, by natural law definition, would view the opportunity to care for a patient with AIDS as a chance to participate in the overall plan of creation and fulfill a set of ultimate goals.
Although such decisions are usually made on a practical, not a theoretical level, at times it is important to be able to relate a decision to its underlying system or principle.
In the course of medical training, physicians are frequently taught to apply a very strict standard in the determination of a patient's capacity or ability to make decisions. A framework for ethical decision making presupposes that physicians making decisions know that a system of ethics exists, the content of that ethical system, and that the system applies to similar decision-making problems despite the multiple variables. As an example, many institutions have adopted policies that do not allow a medicated patient to sign consent forms within a specified time. But the chronic pain management patient on continuous high-dose opioid pain control may not have the capacity of reason.
From an ethical point of view, the patient is a capable decision maker if he or she can understand information relevant to the decision at hand, interact and communicate with caregivers about the decision, and weigh the possible alternatives. A general checklist upon which to set up an ethical framework comes from the Handbook for Hospital Ethics Committees. One might abide by the following steps [18]:
Collection of a database
Case presentation
Identification of medical problems
Identification of psychological problems
Identification of an ethical dilemma
Identification of legal or policy issues
Discussion of ethical issues
Suggestions for approaches to problems
Discussion with initiator, patient, if possible, and other individuals directly involved with specific patient or problem
Documentation of issues discussed and suggested approaches to be placed in the patient's chart
Whenever possible, the patient or family makes the final healthcare decision. The first and most important step is the collection of a database, which involves gathering and assessing the facts. The nursing staff can be instrumental in facilitating the stages of ethical action. The following is a general outline of each step and the process that develops as one moves through the individual stages. In each step, questions are offered to help the healthcare professional gather all the information necessary to assist the patient and healthcare team in the decision-making process.
It is important to note that using professional interpreters for patients with limited English proficiency will help ensure quality care. Convenience and cost lead many clinicians to use "ad hoc" interpreters (e.g., family members, friends, bilingual staff members) instead of professional interpreters. However, professional interpreters are preferred for several reasons. Several states have laws about who can interpret medical information for a patient, so healthcare professionals should check with their state's health officials about the use of ad hoc interpreters [19]. Even when allowed by law, the use of a patient's family member or friend as an interpreter should be avoided, as the patient may not be as forthcoming with information and the family member or friend may not remain objective [19]. Children should especially be avoided as interpreters, as their understanding of medical language is limited, and they may filter information to protect their parents or other adult family members [19]. Individuals with limited English language skills have actually indicated a preference for professional interpreters rather than family members [20].
Most important, perhaps, is the fact that clinical consequences are more likely with ad hoc interpreters than with professional interpreters [21]. A systematic review of the literature showed that the use of professional interpreters facilitates a broader understanding and leads to better clinical care than the use of ad hoc interpreters, and many studies have demonstrated that the lack of an interpreter for patients with limited English proficiency compromises the quality of care. The use of professional interpreters improves communication (errors and comprehension), utilization, clinical outcomes, and patient satisfaction with care [20,22]. One review of case studies regarding professional interpretation noted that "patients with limited English proficiency in the United States have a legal right to access language services, and clinicians have legal and ethical responsibilities to communicate through qualified interpreters when caring for these patients" [23].
Every decision takes some thought and organization before a conclusion may be reached. To create an atmosphere in which effective decisions can be made and implemented, the following is helpful, even in a crisis situation:
Create an atmosphere of caring as you deliberate. Identify those involved with the ethical dilemma and involve them in the decision making when appropriate. Listen to their remarks before proceeding.
Be aware of your personal prejudices and feelings as you respond. Be honest with yourself about how those factors can affect your decision-making ability.
For decisions about foregoing treatment or other dilemmas, the following questions may be relevant, although this list is not exclusive by any means.
What is the patient's current medical status?
Are there other contributing medical conditions?
What is the diagnosis? The prognosis? How reliable are these?
Has a second opinion been obtained? Would it be helpful?
Are there other tests that could clarify the situation?
What treatments are possible?
What is the probable life expectancy and what will be the general condition if treatment is given?
What are the risks and side effects of treatment?
What is the probability that treatment will benefit the patient?
What benefits will treatment provide?
Is the patient competent? Does he or she understand the need for medical care, the options that are available, and the probable results of choosing each of the various available courses of action?
Has the patient been informed about his or her condition?
How was the patient informed?
Have all the treatment alternatives and their possible consequences been discussed with the patient?
Has the patient had time to reflect upon the situation and upon the possible options?
Has the patient made a clear statement about his or her wishes? If so, what are they?
Has the patient discussed the situation thoroughly with someone other than the members of the immediate healthcare team?
If the patient is not currently competent, is he or she expected to regain competence?
If the patient is incompetent, did he or she ever make a clear statement that would indicate his or her wishes in these circumstances?
Is there an advance directive for this patient, and is it available to the healthcare team?
If the patient has not made any clear statement and does not have an advance directive, is there information from anyone regarding what the patient might have wanted or might reasonably be assumed to have wanted?
Are there family members and who are they? Are they available to the healthcare team?
Do they fully understand the patient's condition?
What are their positions?
Do they agree with one another?
Are there any reasons to question their motives?
Has one person been identified as having the primary responsibility for communication and decision making?
Does anyone have legal custody of the patient (guardianship)?
If the patient is a minor, are the legal guardian(s) choosing a course of action that is clearly in the child's best interests?
If there are problems in communicating with the family, can someone be found (e.g., translator, minister) who could be helpful as a liaison between the family and the healthcare team?
Are the caregivers fully apprised of the facts?
What are their views?
If the caregivers disagree, what accounts for the disagreements? Can they be resolved?
Are there state statutes or case law that apply to this situation?
What potential liability might be present with respect to the hospital, to the providers, and to the parent or guardian?
Are there hospital policies or guidelines that apply, and would they be helpful in this situation?
Are there other persons (in or outside the institution) who should be given information or asked for an opinion?
Would it help to consult the literature for any aspect of this case?
Is expense to the patient and/or family a factor?
There are five fundamental components to the cognitive decision-making process as identified by ethicists Kenyon and Congress. They encompass naming the dilemma, sorting the issues, solving the problem, acting, and evaluating and reflecting [10,15]:
Naming the dilemma involves identifying the values in conflict. If they are not ethical values or principles, it is not truly an ethical dilemma. It may be a communication problem or an administrative or legal uncertainty. The values, rights, duties, or ethical principles in conflict should be evident, and the dilemma should be named (e.g., this is a case of conflict between patient autonomy and doing good for the patient). This might happen when a patient refuses an intervention or treatment that the physician thinks would benefit the patient. When principles conflict, such as those in the example statement above, a choice must be made about which principle should be honored.
Sort the issues by differentiating the facts from values and policy issues. Although these three matters often become confused, they need to be identified, particularly when the decision is an ethical one. So, ask the following questions: what are the facts, values, and policy concerns, and what appropriate ethical principles are involved for society, for you, and for the involved parties in the ethical dilemma?
Solve the problem by creating several choices of action. This is vital to the decision-making process and to the patient's sense of controlling his or her life. When faced with a difficult dilemma, individuals often see only two courses of action that can be taken. These may relate to choosing an intervention, dealing with family and friends, or exploring available resources. It is good to brainstorm about all the possible actions that could be taken (even if some have been informally excluded). This process gives everyone a chance to think through the possibilities and to make clear arguments for and against the various alternatives. It also helps to discourage any possible polarization of the parties involved. Ethical decision making is not easy, but many problems can be solved with creativity and thought. This involves the following:
Gather as many creative solutions as possible by brainstorming before evaluating suggestions (your own or others).
Evaluate the suggested solutions until you come up with the most usable ones. Identify the ethical and political consequences of these solutions. Remember that you cannot turn your ethical decision into action if you are not realistic regarding the constraints of institutions and political systems.
Identify the best solution. Whenever possible, arrive at your decision by consensus so that others will support the action. If there are no workable solutions, be prepared to say so and explain why. If ethics cannot be implemented because of politics, this should be discussed. If there are no answers because the ethical dilemma is unsolvable, the appropriate people also must be informed. Finally, the patient and/or family should be involved in making the decision, and it is imperative to implement their choice.
Initiate and act because ethics without action is just talk. In order to act, make sure that you communicate what must be done. Share your individual or group decision with the appropriate parties and seek their cooperation. Implement the decision.
Evaluate and reflect, as perfect ethical decisions are seldom possible. However, healthcare professionals can learn from past decisions and try to make them better in the future, particularly when they lead to policy making. To do this:
Review the ramifications of the decision.
Review the process of making the decision. For example, ask yourself if you would do it in the same way the next time and if the appropriate people were involved.
Ask whether the decision should become policy or if more cases and data are needed before that step should occur.
Learn from successes and errors.
Be prepared to review the decision at a later time if the facts or issues change.
Many physicians have known an old, wise, and respected clinical colleague who told of helping patients with terminal cancer in intractable pain "go more easily (and quickly) with a bit of extra morphine sulfate." Of course, this action was performed quietly, with permission from the patient and/or his or her family (not written) and the tacit understanding of the nursing staff. This is in contradistinction to the retired pathologist Dr. Jack Kevorkian, who flagrantly performed an assisted suicide on a patient with national television coverage in 1998. He was subsequently convicted of second-degree murder for the act and sentenced to 10 to 25 years in prison. In October 2002, the U.S. Supreme Court rejected his appeal to overturn the verdict. As will be discussed, in 1997 the Court had previously decided that there is no constitutional right to physician-assisted suicide.
The physician-assisted suicide debate, like the abortion issue, is many sided, with differing opinions from members of all religious and cultural groups. What is somewhat unusual is that the subject has appeared on the ballots in some states to allow the voting public to cast an opinion. However, as noted, the judiciary's opinion in the matter often leads to the final decision. There are two court cases that are of major importance in this matter; they are the cases of Dennis Vacco v. Timothy Quill, MD, et al. in New York and the State of Washington v. Glucksberg.
On June 26, 1997 the U.S. Supreme Court decided these two cases, reversing the landmark court of appeals decisions that had invalidated laws in New York and Washington that criminalize physician-assisted suicide [24].
In March 1996, the Ninth Circuit Court of Appeals had concluded in Compassion in Dying v. State of Washington (now titled State of Washington v. Glucksberg) that there is a constitutionally protected liberty interest in determining the time and manner of one's own death. It then ruled that a Washington state law prohibiting physicians from prescribing life-ending medication for use by terminally ill, competent adults violates this Fourteenth Amendment due process right [24].
The Second Circuit Court of Appeals in Quill v. Vacco, invalidating New York's similar law on a narrower ground, concluded that the statute violated the equal protection rights of mentally competent, terminally ill persons. Given that those on life support systems are permitted to hasten their deaths by having their doctors take them off life support, the court found no reason to prohibit those in the final stages of their illnesses who are not on life support from making the same choice by requesting lethal medication from their physicians [25].
In opinions authored by former Chief Justice Rehnquist, the Supreme Court rejected the argument that the state statutes outlawing assisted suicide infringed upon any fundamental right, and concluded that, because all competent persons are entitled to refuse lifesaving medical treatment and no one is permitted to assist a suicide, that there was no different treatment of similarly situated persons to trigger the Equal Protection Clause of the Fourteenth Amendment [24].
Although all nine justices agreed with the result, there was observation that this result "permits the debate [about assisted suicide] to continue, as it should in a democratic society" [24]. A majority of the justices made it clear that after public debate and legislative consideration have run a reasonable course, they might rule differently in a different case at a later time [25]. It is interesting that in both of these cases the plaintiffs included physicians and terminally ill patients who desired to overturn state statutes that made it illegal for physicians to assist patients in ending their lives.
Some states, most notably Oregon, have used voter initiatives to attempt to change the law. In January 2006, the Supreme Court upheld Oregon's 1997 Death with Dignity Act (DWDA), a unique initiative that allows physicians to prescribe lethal doses of prescription medicines to patients diagnosed with a terminal illness that will lead to death within six months [26]. As it now stands, a patient may make a written request that medication be prescribed to end his or her own life. There must be two witnesses to attest that the patient is competent, one of which shall not be a family member; the attending physician also may not be a witness. No criminal, civil, or disciplinary action may be brought against any person involved in implementing or witnessing the act. The Act requires the Oregon Health Authority to collect information about patients and physicians who participate in the Act. In 2024, 376 people had died from ingesting the prescribed medications. This number included 43 patients who had received physician prescriptions in previous years [27].
The American Medical Association (AMA) published its first Code of Medical Ethics in 1847, shortly after establishment of the organization that same year [28]. The AMA Council on Ethical and Judicial Affairs (CEJA)—composed of seven practicing physicians, one fellow or resident, and one medical student—is responsible for developing, maintaining, and updating the AMA's ethical guidelines to keep pace with the evolution of medicine and healthcare practice. It also promotes adherence to the Code's professional ethical standards [29]. The Code is updated periodically to address the changing conditions of medicine. The current edition, adopted in June 2016, is the culmination of an eight-year project to comprehensively review, update, and reorganize guidance to ensure that the Code remains a timely, easy-to-use resource. The Code is accessible online at the AMA website and may be downloaded or purchased in book form.
The "Principles of Medical Ethics" is the first section of the current AMA Code and outlines basic standards of practice [30].
The medical profession has long subscribed to a body of ethical statements developed primarily for the benefit of the patient. As a member of this profession, a physician must recognize responsibility to patients first and foremost, as well as to society, to other health professionals, and to self. The following Principles adopted by the American Medical Association "are not laws, but standards of conduct that define the essentials of honorable behavior for the physician" [30].
A physician shall be dedicated to providing competent medical care, with compassion and respect for human dignity and rights.
A physician shall uphold the standards of professionalism, be honest in all professional interactions, and strive to report physicians deficient in character or competence, or engaging in fraud or deception, to appropriate entities.
A physician shall respect the law and also recognize a responsibility to seek changes in those requirements that are contrary to the best interests of the patient.
A physician shall respect the rights of patients, colleagues, and other health professionals, and shall safeguard patient confidences and privacy within the constraints of the law.
A physician shall continue to study, apply, and advance scientific knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues, and the public, obtain consultation, and use the talents of other health professionals when indicated.
A physician shall, in the provision of appropriate patient care, except in emergencies, be free to choose whom to serve, with whom to associate, and the environment in which to provide medical care.
A physician shall recognize a responsibility to participate in activities contributing to the improvement of the community and the betterment of public health.
A physician shall, while caring for a patient, regard responsibility to the patient as paramount.
A physician shall support access to medical care for all people.
Following the Preamble, the AMA Code of Medical Ethics provides guidance ("Opinions") on ethical practice across 11 domains, or chapters:
Patient-Physician Relationships
Consent, Communication, and Decision Making
Patient Privacy and Confidentiality
Genetics and Reproductive Medicine
Palliative and End of Life Care
Organ Procurement and Transplantation
Research and Innovation
Physicians and the Health of the Community
Professional Self-Regulation
Interpersonal Relationships
Financing and Delivery of Health Care
Each chapter addresses a range of clinical and societal issues, situations, and potential conflicts pertaining to current medical practice. By way of example, and to illustrate the tone and applicability of the guidance provided, selected excerpts (subsections) from the AMA Code of Ethics are reproduced below, with permission [31].
The practice of medicine, and its embodiment in the clinical encounter between a patient and a physician, is fundamentally a moral activity that arises from the imperative to care for patients and to alleviate suffering. The relationship between a patient and a physician is based on trust, which gives rise to physicians' ethical responsibility to place patients' welfare above the physician's own self-interest or obligations to others, to use sound medical judgment on patients' behalf, and to advocate for their patients' welfare.
A patient-physician relationship exists when a physician serves a patient's medical needs. Generally, the relationship is entered into by mutual consent between physician and patient (or surrogate).
However, in certain circumstances a limited patient-physician relationship may be created without the patient's (or surrogate's) explicit agreement. Such circumstances include:
When a physician provides emergency care or provides care at the request of the patient's treating physician. In these circumstances, the patient's (or surrogate's) agreement to the relationship is implicit.
When a physician provides medically appropriate care for a prisoner under court order, in keeping with ethics guidance on court-initiated treatment.
When a physician examines a patient in the context of an independent medical examination, in keeping with ethics guidance. In such situations, a limited patient-physician relationship exists.
The health and well-being of patients depends on a collaborative effort between patient and physician in a mutually respectful alliance. Patients contribute to this alliance when they fulfill responsibilities they have, to seek care and to be candid with their physicians.
Physicians can best contribute to a mutually respectful alliance with patients by serving as their patients' advocates and by respecting patients' rights. These include the right:
To courtesy, respect, dignity, and timely, responsive attention to his or her needs.
To receive information from their physicians and to have opportunity to discuss the benefits, risks, and costs of appropriate treatment alternatives, including the risks, benefits, and costs of forgoing treatment. Patients should be able to expect that their physicians will provide guidance about what they consider the optimal course of action for the patient based on the physician's objective professional judgment.
To ask questions about their health status or recommended treatment when they do not fully understand what has been described and to have their questions answered.
To make decisions about the care the physician recommends and to have those decisions respected. A patient who has decision-making capacity may accept or refuse any recommended medical intervention.
To have the physician and other staff respect the patient's privacy and confidentiality.
To obtain copies or summaries of their medical records.
To obtain a second opinion.
To be advised of any conflicts of interest their physician may have in respect to their care.
To continuity of care. Patients should be able to expect that their physician will cooperate in coordinating medically indicated care with other healthcare professionals, and that the physician will not discontinue treating them when further treatment is medically indicated without giving them sufficient notice and reasonable assistance in making alternative arrangements for care.
Protecting information gathered in association with the care of the patient is a core value in health care. However, respecting patient privacy in other forms is also fundamental, as an expression of respect for patient autonomy and a prerequisite for trust.
Patient privacy encompasses a number of aspects, including personal space (physical privacy), personal data (informational privacy), personal choices including cultural and religious affiliations (decisional privacy), and personal relationships with family members and other intimates (associational privacy).
Physicians must seek to protect patient privacy in all settings to the greatest extent possible and should:
Minimize intrusion on privacy when the patient's privacy must be balanced against other factors.
Inform the patient when there has been a significant infringement on privacy of which the patient would otherwise not be aware.
Be mindful that individual patients may have special concerns about privacy in any or all of these areas.
Be transparent with any inquiry about existing privacy safeguards for patient data but acknowledge that anonymity cannot be guaranteed and that breaches can occur notwithstanding best data safety practices.
Relationships among physicians and professional medical organizations and pharmaceutical, biotechnology, and medical device companies help drive innovation in patient care and contribute to the economic well-being of the community to the ultimate benefit of patients and the public. However, an increasingly urgent challenge for both medicine and industry is to devise ways to preserve strong, productive collaborations at the same time that they take clear effective action to prevent relationships that damage public trust and tarnish the reputation of both parties.
Gifts to physicians from industry create conditions that carry the risk of subtly biasing—or being perceived to bias—professional judgment in the care of patients.
To preserve the trust that is fundamental to the patient-physician relationship and public confidence in the profession, physicians should:
Decline cash gifts in any amount from an entity that has a direct interest in physicians' treatment recommendations.
Decline any gifts for which reciprocity is expected or implied.
Accept an in-kind gift for the physician's practice only when the gift will directly benefit patients, including patient education, and is of minimal value.
Academic institutions and residency and fellowship programs may accept special funding on behalf of trainees to support medical students', residents', and fellows' participation in professional meetings, including educational meetings, provided the program identifies recipients based on independent institutional criteria and funds are distributed to recipients without specific attribution to sponsors.
Familiarity with and adherence to the AMA Code of Medical Ethics can offer a degree of protection from the various pitfalls of practicing medicine in contemporary American society, such as administrative sanctions and malpractice suits. Following federal, state, and local laws, along with any/all ethical codes or rules where practicing, offers further protection from legal or administrative action; however, ethical medical principles are primarily intended to benefit the patient during their time of uncertainty. The goal of ethics, and ethical practice, is to do right by the patient, avoid harm, and maintain trust with the patient and the public, so essential to the humane and safe practice of medicine. The physician with a good understanding of ethics is equipped to serve the patient well; to listen, inform, and provide a measure of autonomy; and, when necessary, confront difficult choices or ethical dilemmas with the confidence required to make sound decisions.
| Journal of Bioethics |
| https://bioethicstoday.org |
| AMA Ethics |
| https://www.ama-assn.org/about/ethics |
1. Rothman DJ. Strangers at the Bedside: A History of How Law and Bioethics Transformed Medical Decision Making. New York, NY: Basic Books; 1991.
2. Monette DR, Sullivan TJ, DeJong CR, Hilton TP. Applied Social Research: A Tool for Human Services. 9th ed. Belmont, CA: Brooks/Cole; 2014.
3. U.S. Department of Health and Human Services. The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research. Available at https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/index.html. Last accessed December 9, 2025.
4. The Hastings Center for Bioethics. Available at https://www.thehastingscenter.org. Last accessed December 9, 2025.
5. Presidential Commission for the Study of Bioethical Issues. History of Bioethics Commissions. Available at https://bioethicsarchive.georgetown.edu/pcsbi/history.html. Last accessed December 9, 2025.
7. Malcolm AH. Judge Allows Feeding-Tube Removal. Available at https://www.nytimes.com/1990/12/15/us/judge-allows-feeding-tube-removal.html. Last accessed December 9, 2025.
8. Authority: Secs. 1102,1861. 1864. 1866. 1867, and 1871 of the Social Security Act (42 U.S.C. 1302.1395x. 1395aa. 1395cc. 1395dd. and 1395hh) and sec. 602 (k) of Pub. L. 9621 (42 U.S.C 1395ww note).
9. The Joint Commission. 2025 Comprehensive Accreditation Manual for Hospitals. Oakbrook Terrace, IL: Joint Commission Resources; 2024.
10. Kenyon P. What Would You Do? An Ethical Case Workbook for Human Service Professionals. Pacific Grove, CA: Brooks/Cole Publishing Company; 1999.
12. Rushton CH, Hogue EE. Balancing personal risk with professional responsibility: the case of AIDS. Pediatr Nurs. 1993;196(4):415, 418-420.
14. Harper MG. Ethical multiculturalism: an evolutionary concept analysis. ANS Adv Nurs Sci. 2006;29(2):110-124.
15. Congress EP. Social Work Values and Ethics: Identifying and Resolving Professional Dilemmas. Chicago, IL: Nelson-Hall; 1999: 31-33.
16. Pence T, Cantrall J (eds). Ethics in Nursing: An Anthology. New York, NY: National League for Nursing; 1990.
17. Macklin R. Ethical relativism in a multicultural society. Kennedy Inst Ethics J. 1998;8(1):1-22.
18. Ross JW, Bayley C, Michel V, Pugh D. Handbook for Hospital Ethics Committees. Chicago, IL: American Hospital Association; 1986.
19. Sevilla Mátir JF, Willis DR. Using bilingual staff members as interpreters. Fam Pract Manag. 2004;11(7):34-36.
20. Ngo-Metzger Q, Massagli MP, Clarridge BR, et al. Linguistic and cultural barriers to care. J Gen Intern Med. 2003;18(1):44-52.
21. Flores G. Language barriers to health care in the United States. N Engl J Med. 2006;355(3):229-231.
22. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005;62(3):255-299.
23. Basu G, Costa VP, Jain P. Clinicians' obligations to use qualified medical interpreters when caring for patients with limited English proficiency. AMA J Ethics. 2017;19(3):245-252.
25. Grinfeld MJ. Assisted suicide: just how far did the Supreme Court go. Psychiatric Times. 1997;14(8).
26. Oregon Health Authority. Oregon's Death with Dignity Act. Available at https://www.oregon.gov/oha/ph/ProviderPartnerResources/EvaluationResearch/DeathwithDignityAct/Pages/index.aspx. Last accessed December 9, 2025.
27. Oregon Health Authority. 2024 Oregon Death with Dignity Act: Data Summary. Available at https://www.oregon.gov/oha/PH/PROVIDERPARTNERRESOURCES/EVALUATIONRESEARCH/DEATHWITHDIGNITYACT/Documents/year27.pdf. Last accessed December 9, 2025.
28. American Medical Association. AMA History. Available at https://www.ama-assn.org/about/ama-history/ama-history. Last accessed December 9, 2025.
29. American Medical Association. Council on Ethical and Judicial Affairs. Available at https://www.ama-assn.org/about/council-ethical-judicial-affairs. Last accessed December 9, 2025.
30. American Medical Association. Code of Medical Ethics. AMA Principles of Medical Ethics. Available at https://code-medical-ethics.ama-assn.org/principles. Last accessed December 9, 2025.
31. American Medical Association. Code of Medical Ethics. Chapters. Available at https://code-medical-ethics.ama-assn.org/chapters. Last accessed December 11, 2025.
Mention of commercial products does not indicate endorsement.